Hand Eczema
HAND ECZEMA: Symptoms, Types, Treatment and Daily Care
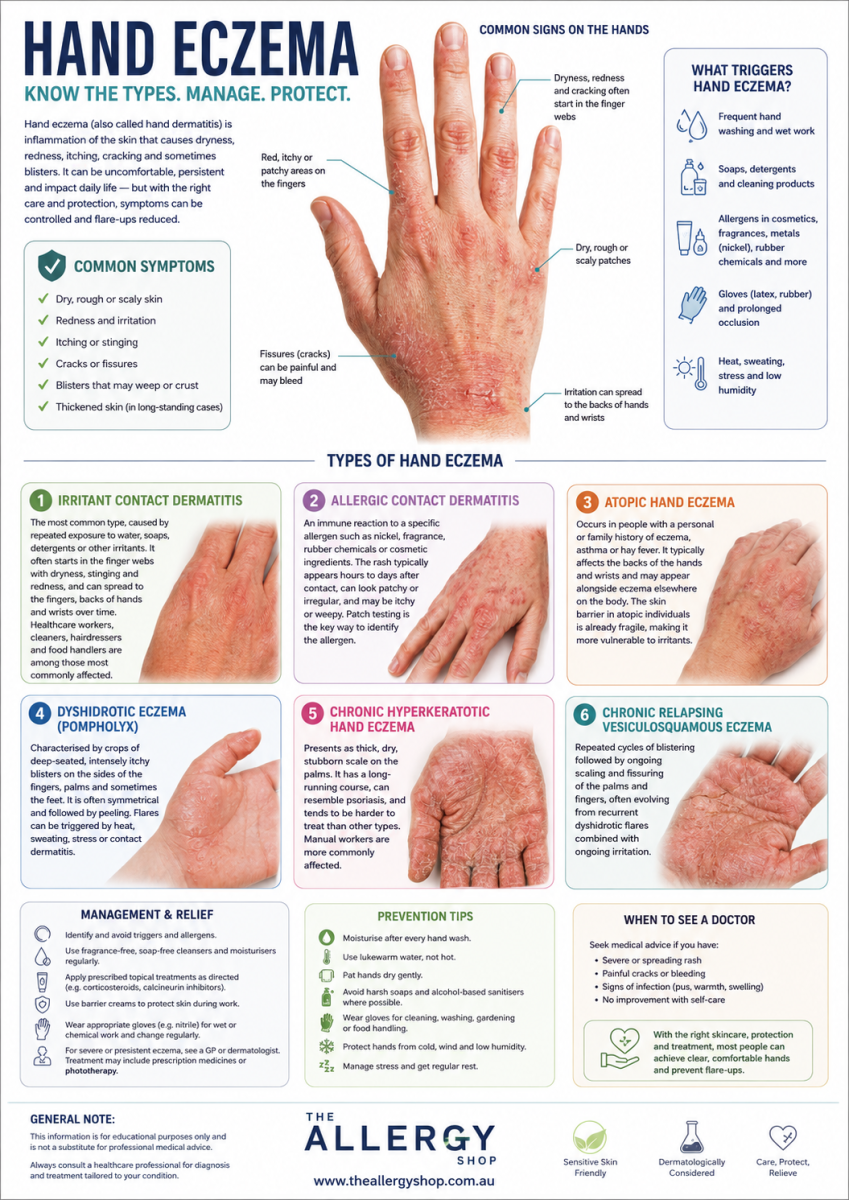
Click HERE for a Visual Guide to the Main Symptoms and Types of Hand Eczema
{kind=link}
What is hand eczema? Hand eczema (also called hand dermatitis) is a common inflammatory skin condition that affects the hands, causing dryness, redness, itching, blisters, painful cracks or soreness. It is one of the most frequently seen skin conditions in both clinical and occupational settings. It is not contagious and cannot be passed from person to person.
Most cases involve a mix of causes rather than one single trigger. A weakened skin barrier, repeated irritant exposure (such as wet work or detergents), a contact allergy to a specific substance, or an atopic (eczema-prone) background can all contribute — and in many people, more than one of these factors is present at the same time. This overlap is why hand eczema can be persistent and why treatment often needs to address more than one cause.
What are the symptoms of hand eczema? Symptoms vary depending on the type and severity, but commonly include:
- Dryness, tightness and flaking skin
- Redness and swelling
- Itching or burning
- Small fluid-filled blisters
- Weeping or crusting during flares
- Painful cracks or fissures, especially on the fingers and palms
- Thickened or rough skin in chronic cases
Symptoms can come and go, with periods of relative calm followed by flare-ups. In some people the condition becomes chronic and requires ongoing management.
What are the main types of hand eczema?
- Irritant contact dermatitis — the most common type, caused by repeated exposure to water, soaps, detergents or other irritants. It often starts in the finger webs with dryness, stinging and redness, and can spread to the fingers, backs of hands and wrists over time. Healthcare workers, cleaners, hairdressers and food handlers are among those most commonly affected.
- Allergic contact dermatitis — an immune reaction to a specific allergen such as nickel, fragrance, rubber chemicals or cosmetic ingredients. The rash typically appears hours to days after contact, can look patchy or irregular, and may be itchy or weepy. Patch testing is the key way to identify the allergen.
- Atopic hand eczema — occurs in people with a personal or family history of eczema, asthma or hay fever. It typically affects the backs of the hands and wrists and may appear alongside eczema elsewhere on the body. The skin barrier in atopic individuals is already fragile, making it more vulnerable to irritants.
- Dyshidrotic eczema (pompholyx) — characterised by crops of deep-seated, intensely itchy blisters on the sides of the fingers, palms and sometimes the feet. It is often symmetrical and followed by peeling. Flares can be triggered by heat, sweating, stress or contact dermatitis.
- Chronic hyperkeratotic hand eczema — presents as thick, dry, stubborn scale on the palms. It has a long-running course, can resemble psoriasis, and tends to be harder to treat than other types. Manual workers are more commonly affected.
- Chronic relapsing vesiculosquamous eczema — repeated cycles of blistering followed by ongoing scaling and fissuring of the palms and fingers, often evolving from recurrent dyshidrotic flares combined with ongoing irritation.
Here types of Hand Eczema:

How is hand eczema treated?
Treatment follows a layered approach, starting with the basics and stepping up when needed:
- Emollients (moisturisers) — the foundation of all hand eczema management. Regular use helps repair the skin barrier, reduces water loss and makes the skin less prone to cracking. Ointments are most effective for very dry or cracked skin; creams are easier for daytime use. Many people use a lighter cream during the day and a greasier ointment at night. Emollients can also be used as a soap substitute to reduce further irritation from washing.
- Topical corticosteroids — the main anti-inflammatory treatment for active flares. Because the skin on the palms is thick, hands often need stronger steroid prescriptions than thinner skin areas. When used as directed, topical steroids are safe and effective; problems typically arise from prolonged unsupervised use rather than correctly prescribed short courses.
- Calcineurin inhibitors (tacrolimus, pimecrolimus) — steroid-sparing anti-inflammatory creams or ointments used when repeated steroid courses are needed or when a non-steroid option is preferred. A mild stinging sensation when first applied usually settles within a few days.
- Phototherapy — clinic-based ultraviolet treatment (typically narrowband UVB or PUVA) for cases that remain active despite good topical care. Given over multiple sessions across several weeks, usually combined with the usual topical routine. Phototherapy: all you need to know about Phototherapy by clicking HERE
- Systemic treatment — reserved for moderate to severe or function-limiting hand eczema under specialist supervision. Options include oral corticosteroids for a severe flare, longer-term agents such as ciclosporin, methotrexate or azathioprine, and targeted biologics such as dupilumab or JAK inhibitors in selected patients. These require monitoring and are chosen on a case-by-case basis.
Here Hand Eczema Treatment:

What triggers hand eczema flares? Understanding your personal triggers is one of the most effective ways to reduce flare frequency. Common triggers include:
- Frequent handwashing and prolonged wet work
- Soaps, detergents, cleaning products and solvents
- Sweating, heat and humid conditions
- Stress
- Specific allergens such as fragrance, nickel, rubber chemicals or cosmetic ingredients
- Workplace exposures (chemicals, gloves, tools)
- Fungal infections (can worsen dyshidrotic eczema in some people)
Keeping a simple diary of flares alongside activities, products and exposures can help identify patterns that are not immediately obvious.
Practical daily tips for managing hand eczema
Reducing irritant exposure is just as important as treating active inflammation. Small, consistent habit changes can make a significant difference over time:
- Moisturise immediately after every handwash, before hands fully dry
- Use a gentle, fragrance-free cleanser instead of regular soap for routine washing where appropriate — note that soap substitutes are not antimicrobial, so use soap or sanitiser when hygiene requires it
- Dry hands thoroughly, patting rather than rubbing
- Wear task-appropriate gloves for wet work, cooking and cleaning; use cotton liners for longer tasks as sweating can worsen eczema
- If you are allergic to latex, choose nitrile gloves instead
- Apply a thick ointment or emollient at night, optionally under cotton gloves, to allow deeper absorption overnight
- Keep a moisturiser beside the sink, at your desk and by the bed so it is always within reach
- Use a dishwasher where possible to reduce direct detergent contact
- At work, ask whether tasks can be rotated to reduce wet work time and whether skin-friendly alternatives to current products are available
When should I see a doctor about hand eczema? It is worth seeing your GP if:
- Symptoms are severe, widespread or getting worse
- The skin is cracked, bleeding or showing signs of infection (increased redness, warmth, pus or swelling)
- Eczema is interfering with work, sleep or daily activities
- Symptoms keep coming back despite basic skincare
- The pattern is unusual, asymmetrical or not responding as expected
Your GP may refer you for patch testing or dermatology review. Patch testing is particularly valuable in chronic, recurrent or work-related hand eczema to identify allergic triggers that are not obvious from the history alone.

What results can I realistically expect? It is important to have realistic expectations. Most treatments control hand eczema rather than permanently cure it. In allergic contact dermatitis, identifying and strictly avoiding the allergen can sometimes lead to major improvement or near-clearance. In chronic irritant, occupational or atopic hand eczema, ongoing maintenance is usually needed to keep symptoms manageable.
The most meaningful goals are calmer skin, fewer cracks, less itch, better sleep, fewer flare-ups and hands that function comfortably for work and daily life. With the right combination of diagnosis, trigger reduction, regular moisturising and appropriate treatment during flares, most people can achieve good day-to-day control.
Frequently asked questions FAQ
- Is hand eczema the same as hand dermatitis? Yes — the two terms are used interchangeably and refer to the same condition.
- Is hand eczema contagious? No. Eczema is an inflammatory skin condition, not an infection, and cannot be passed to others.
- What causes hand eczema most often? The most common drivers are irritants such as water, soaps and detergents from repeated wet work. Allergy to specific substances and an atopic background are also frequent contributors, and many people have a combination of causes.
- What is the difference between irritant and allergic contact dermatitis? Irritant dermatitis is caused by physical damage to the skin from substances like soaps or water. Allergic dermatitis is an immune reaction to a specific substance and typically causes a delayed rash appearing hours to days after contact.
- Why do I get tiny itchy blisters on my hands? This pattern most commonly suggests dyshidrotic eczema (pompholyx), which causes deep-seated itchy blisters on the sides of the fingers and palms.
- Do I need patch testing? Patch testing is worth discussing with your GP or dermatologist if your hand eczema is chronic, recurrent, work-related, asymmetrical or not improving as expected. It is the most reliable way to identify allergic contact triggers.
- What moisturiser is best for hand eczema? A simple, fragrance-free emollient is usually the safest choice. Ointments work best for very dry or cracked skin; creams are more practical for daytime use. If a product stings or appears to worsen the rash, speak to your pharmacist or GP about alternatives.
- Are steroid creams safe to use on the hands? Yes, when used as prescribed. Hands often require a stronger topical steroid than other body areas, particularly on the palms, because the skin is thicker there. Correctly prescribed short courses are considered safe and effective.
- How long does hand eczema take to improve? Mild flares may settle over days to a few weeks with good skin care. Chronic hand eczema often takes longer and may need ongoing maintenance to prevent relapse, especially if triggers continue.
- When should I see a doctor? See your GP if symptoms are severe, painful, infected, persistent, recurrent or affecting your ability to carry out normal activities.
Following Hand Dermatitis a Pocket Guide for Health Care Workers It can be downloaded clicking HERE